Equivalent Child Outcomes in Same-Sex vs. Different-Sex Parent Households
Joan Lipuscek
In the United States, beliefs about child and family outcomes for same-sex versus different-sex parents have been a source of confusion and debate. To address this topic, the Journal of Developmental & Behavioral Pediatrics published the recent study, "Same-Sex and Different-Sex Parent Households and Child Health Outcomes: Findings from the National Survey of Children’s Health" by Henry M. W. Bos et al. This study found no significant difference between outcomes for children raised in similarly stable same-sex versus different-sex parent households. However, the study did find that same-sex parents report significantly higher levels of parenting stress compared to different-sex parents.
METHODS
In this study, the National Survey of Children's Health (NSCH) data set was used to examine 95 female same-sex parent families and 95 different-sex parent families. the NSCH is a population-based survey on children's health. Families were chosen if they were stable and didn’t experience a major stress event such as divorce or separation. In order to participate, two parents had to be presently coupled and had to have raised their children since birth. Same-sex male parents were not selected because there were too few households meeting these criteria. The researchers note that one of the strengths of the investigation was that "the data were drawn from a population-based survey on children's health that was not described to participants as a study of same-sex parent families, thus minimizing potential bias."
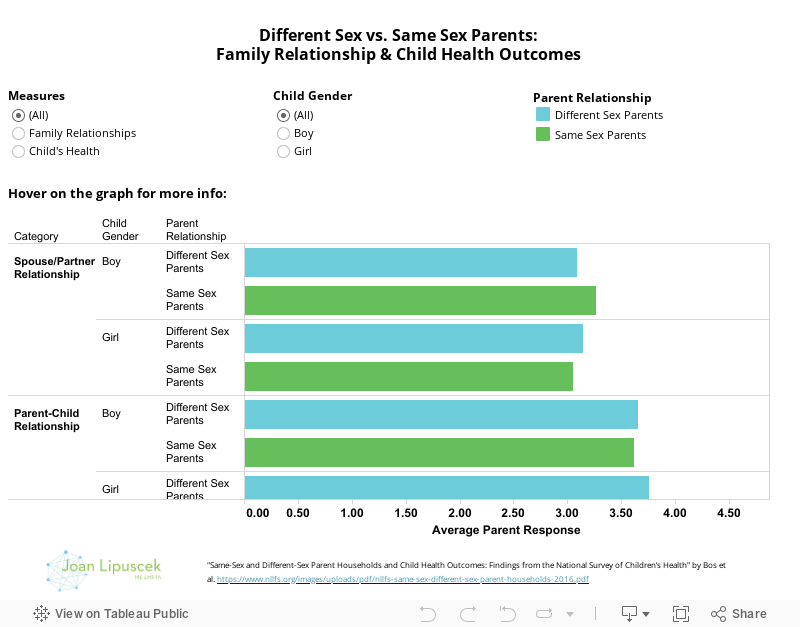
Researchers focused on data from households with children ages 6 through 17 and focused on questions about “family relationships, parenting stress and child outcomes.” This data set offered a chance for the researchers to examine whether there “are there differences in family relationships (spouse/partner relationships and parent-child relationships), parenting stress, or child outcomes (general health, emotional difficulties, coping behavior, and learning behavior)" between same-sex and different-sex parent households.
We have created the following visualization that summarizes the major findings from this study. (Please set your browser to allow third party cookies if you receive an error while trying to explore the data.)
THE RESULTS
The study findings illustrate that there is no significant difference between same-sex and different-sex parent households in terms of spouse/partner relationship, parent/child relationship, child general health, child emotional difficulties, child coping behavior and child learning behavior. Thus, the researchers conclude that this study "contributes to the mounting evidence that children reared by same-sex parents fare at least as well as those reared by different-sex parents on a variety of measures used to assess psychological adjustment."
The one exception to these otherwise equivalent results, however, was that the same sex couples reported experiencing greater parenting stress. At this point in time little is known as to why same-sex parents experience greater stress as parents, but one theory suggests that the "cultural spotlight on child outcomes in families with same sex-parents” may be a causally contributing to the stress.
Typically, greater parenting stress is a predictor that is "positively associated with children's emotional difficulties and negatively associated with child coping and learning behavior." Interestingly, however, greater parenting stress in same-sex parents did not manifest in these negative results. In an attempt to explain this, the researchers hypothesize that lesbian mothers are mitigating greater parenting stress by effectively utilizing support systems such as parenting groups and counseling services to allay negative child outcomes.
ADVICE FOR PARENTS
Unfortunately, homophobia in society and concerns about how societal attitudes may impact their families may be contributing to excess parenting stress among same-sex parents. These parents may also feel the pressure of other people judging them more closely and more critically compared to different-sex parents.
Despite the societal challenges for same-sex parents, challenging days with children are common for all parents alike. Parenting stress can be alleviated by understanding the triggers that contribute to your anxiety throughout the day. For example, you might feel stressed if your child is having a tantrum in a public place, especially if people begin to stare. Instead of saying, “I am a terrible parent because my child is acting out” try adjusting your self-talk to phrases such as: “my child is having a bad day,” “my child is hungry or tired” or “I am doing the best that I can." It is impossible to avoid all stressful parenting situations, but one key is to understand your limitations and allow yourself more time to accomplish tasks.
Also, attempt to prioritize the duties and responsibilities in your day so that you don’t become overwhelmed while setting healthy boundaries with others. Making time for yourself by eating healthy foods, getting enough sleep and daily exercise may also be beneficial. Finally, forming close emotional connections with family members, friends and cultivating a strong support system can also contribute to a healthier lifestyle. If you find that you are not able to deal effectively with the level of stress in your life or if you find that it is getting in the way of effective parenting, it may be time to contact a professional.